

Healthy greetings, Friends of TVD!
Here we are, the fourth issue of CV🦠News! Again, thank you to all five physicians at The Village Doctor for their brainstorming and contribution to this newsletter effort, thank you Drs. Abrams, Phillips, Pittson, and Sangani. Let me again give thanks to the various contributors to our Hope and Grace page, a collection of works and perspectives gathered from around the world.
Also, please NOTE that our Coronavirus FAQ page has undergone a substantial revision, with new formatting, and improved search functionality to help you find the answers to all your burning COVID-19 questions. Have a look here!
HOME ALONE? AT LEAST ANOTHER MONTH…
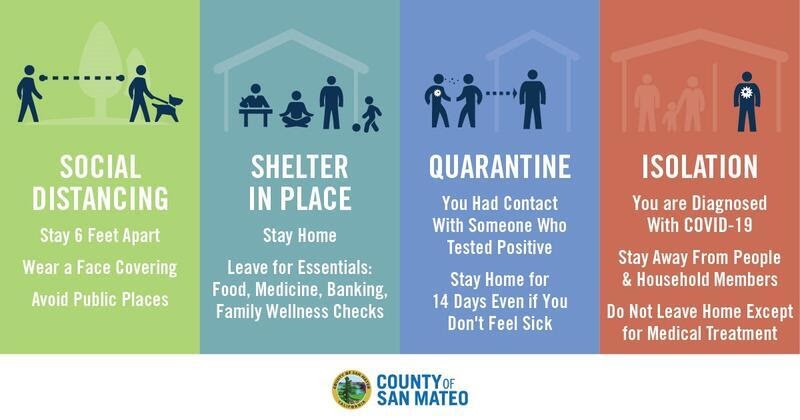
CONTINUE #STAYHOMESAVELIVES. April 29, 2020- Today, health officers in seven Bay Area jurisdictions released orders to extend the previous stay-at-home order through May 31 with some loosening of restrictions. Earlier this week, they released a statement saying “At this stage of the pandemic it is critical that our collective efforts continue so that we do not lose the progress we have achieved together. Hospitalizations have leveled, but more work is needed to safely re-open our communities. Prematurely lifting restrictions could easily lead to a large surge in cases.” As of today, there are 7,273 confirmed cases of COVID-19 and 266 deaths in those seven areas, up from 258 confirmed cases and 4 deaths when the shelter in place order was first issued.
With the new order, the stay-home mandate, social distancing and masking measures remain, but some restrictions on several kinds of businesses and outdoor activities are lifted. Construction projects, landscaping, gardening, golf and tennis will be allowed. Similar to what Governor Newsom discussed last week, any future loosening will be based on five indicators: flattening or decreasing coronavirus case numbers, sufficient hospital capacity, whether the region is meeting the need for testing, stronger contact tracing and isolation, and an adequate supply of PPE for health care workers.

WHAT ABOUT THE COSTS (AND BENEFITS?) OF BEING HOME ALONE?
When can we start reopening our community and getting back to business?
This is a complicated and important question with significant economic, political, and public health components. Today’s Internal Medicine Grand Rounds at Stanford (April 29, 2020) started to talk about this and what follows are some abbreviated notes shared by our own Dr. Jennifer Abrams.
Community “reopening” will be staged, with specific criteria for moving on to the next stage. Availability of widespread testing is necessary as an early warning system. To have adequate monitoring, a Harvard report suggests 5 million tests per day will need to be available by early June and 20 million per day by July. We also need public health capacity to sufficiently trace contacts, isolate and quarantine people. Andy Slavitt, a former director of Medicare and Medicaid in the Obama administration and Scott Gottlieb, a former FDA chief for President Trump, proposed to the government that $47 billion is needed to do this adequately.
We are entering the “end of the beginning phase” of the crisis. Testing will be a key piece of the reset – with the potential to help us move away from blanket restrictions to policy that is more calibrated to risk. Current serology testing continues to have significant scientific uncertainty with respect to immunity along with test quality problems. It is a prudent approach to STOP using the results of current serology testing to influence policy for now. More than 100 serology tests have been submitted to the FDA for review. Many of them are foreign-manufactured, with aggressive marketing and less aggressive science. There is growing evidence of poor accuracy of these tests. Chile is issuing immunity certification “passports” while Germany, the UK, Italy & the Trump administration are considering issuing them. Note that the WHO has recommended against them. Regardless of what the US government decides to do, the private sector may move forward with them to enable people to come back to work, so we should understand the limitations. There are legal, ethical, and policy concerns with immunity certification programs: inequitable access to testing, discrimination based on disease status, racial and socioeconomic disparities, fraud & intentional infection, standardless testing. There is some precedent and courts have generally endorsed immunity certification programs when risk is substantial (e.g. travel requirements & documentation, e.g. yellow fever immunization).
What about the economic and social COSTS of Sheltering in Place (SIP)? Social cost-benefit analysis (“SCBA”) is a common framework for policy evaluation. SCBA requires developing a full list of benefits and harms for everyone in the society, then translates all benefits and harms into monetary units to enable comparison across very different domains and across people. One can then choose to adopt policy if the benefits are greater than the harms. For example: a paper written recently for the National Bureau of Economic Research (NBER) estimates that over four weeks of shelter in place in California, 1,661 deaths were averted, but 400 jobs were lost per life saved. SCBA would translate both into a monetary value and when the cost is greater than the benefit policy makers can argue for a change. However this can only be done when we know enough to make accurate assumptions for SCBA. In the early days of SIP we simply did not know enough.
It is also very important to be clear about the policy being considered and its alternatives. For example, in March 2020 the calculation was between shelter in place versus an unmitigated pandemic. Today it’s whether to continue SIP versus re-open the economy. The key questions that have to be answered are have test & testing capacity increased enough, and how manageable are the economic consequences?
The intended benefits of SIP are reduction in COVID-related mortality and morbidity, and preventing the collapse of the health care system. The unintended benefits are fewer deaths from accidents and pollution, and learning new methods to work from home. The harms of SIP include: health-related, eg. foregoing medical care, and increases in domestic violence, isolation, stress, and economic worries i.e. “deaths of despair”; economy-related, eg. unemployment, loss of savings, bankruptcy of business, recession, large increase in government debt, and loss in tax revenue that funds social programs, and; human capital, eg. missed school, students entering into a weak labor market.
How does one assign a monetary value to a human life? From one of today’s participants, “That is probably the most important question that policy-makers have to confront here. The short answer is yes, lots of agencies use monetary values for decline in mortality risk. Most frequently used by the EPA for environmental policies. EPA currently recommends that the central estimate of $7.4 million ($2006)”. Note this central estimate is a statistical value based on the total dollar amount that a group would be willing to pay to save one statistical life in a year. This is what is meant by the “value of a statistical life.” Importantly, this is not an estimate of how much money any single individual or group would be willing to pay to prevent the certain death of any particular person. (You can read more about Mortality Risk Valuation on the EPA website here).
 RECENT NEWS – MORE ABOUT BLOOD TESTING
RECENT NEWS – MORE ABOUT BLOOD TESTING
Can the serology lab prove that you’re immune to COVID and if so, will we have to carry “immunity passports” to show our status? To date, no study has evaluated whether the presence of antibodies to SARS-CoV-2 confers immunity to subsequent infection. It is not clear if you can get COVID-19 twice. (April 28, 2020). The idea of issuing some form of certificate or passport that could enable those with antibodies to SARS-CoV-2 to resume normal activities has been in the news recently. In a scientific brief from April 24th, 2020, the WHO warns, “At this point in the pandemic, there is not enough evidence about the effectiveness of antibody-mediated immunity to guarantee the accuracy of an ‘immunity passport’ or ‘risk-free certificate.’ People who assume that they are immune to a second infection because they have received a positive test result may ignore public health advice. The use of such certificates may therefore increase the risks of continued transmission.” The WHO also makes the point that serology (antibody) tests need further validation to determine their accuracy and reliability. These tests also need to accurately distinguish between past infection from SARS-CoV-2 and that caused by the known set of six human coronaviruses, four of which cause the common cold and circulate widely. People infected by any one of these viruses may produce antibodies that cross-react with antibodies produced in response to infection with SARS-CoV-2. (See WHO Scientific Brief). Until we have a better understanding of the accuracy and reliability of antibody tests and what a positive antibody test means in terms of immunity to subsequent infection, it is too early to consider immunity passports as a way to loosen social distancing and other infection control measures for some members of the population.
 THE CURVE IS STILL FLAT, AND MORE GOOD NEWS?
THE CURVE IS STILL FLAT, AND MORE GOOD NEWS?
I heard recent testing in the community is showing more people may have been infected than we realized – does that mean the death rate may be lower than we realized?
We know that coronavirus can cause mild and even asymptomatic infections in many people. Antibody testing, also referred to as serology testing, can help inform our understanding of coronavirus infection prevalence and identify those who have already been exposed. An interesting study out of Stanford recruited 3300 residents of Santa Clara County for serology testing over the weekend of April 3rd to estimate the percentage of the county that had been infected with COVID. The study estimates as many as 81,000 people could have been infected, or between 2.5 to 4.2% of residents. If true, this would suggest the death rate may actually be much lower than previously thought. The study, which is still in pre-publication phase, has received a lot of criticism, mostly focused on biases in recruitment (which was done through social media platforms such as Facebook and was likely subject to bias – patients most worried about prior symptoms would be more likely to sign up) and on the error rates of the test kits used (even a small false positive rate could account for much of the findings – while the study authors argue they controlled for the known false positive rate of the test in their projections, many statisticians feel this was not adequate). We are eager to review additional information the study authors plan to release this week and agree that more studies are needed to provide a reliable picture of community prevalence.

MORE CLINICAL THOUGHTS – OXYGEN
What is a pulse oximeter and should I have one at home?
A pulse oximeter is a little device that clips on to the end of your finger and measures your blood oxygen saturation. It uses two wavelengths of light (*see next FAQ on iPhone apps) and magical algorithms to report a percentage. Greater than 93% is good. You’ve likely had your oxygen saturation measured many times in your doctor’s office during routine pre-visit “vital signs.” But these little devices can be finicky, especially when used on cold or small (<10-12 years old) fingers, or those with painted fingernails. One also has to remain still for the device to capture a “good waveform,” which you can see as a bouncing column of LED’s on the display (if the LED’s aren’t bouncing, the reading is not a reliable measurement). All this to say, if anything isn’t quite right, it can report a falsely low oxygen saturation which can worry the inexperienced user, and could lead to unnecessary trips to the ED or calls to strained doctor office phone lines. If you are comfortable using a pulse oximeter, though, I think they are a great additional tool to have when remotely consulting your doctor about if, or when, further evaluation are warranted. But if you’re someone who gets anxious about changing the television input to get to the Roku, you may not want the potential worry or frustration of this particular tool, or its $50 price tag.
I hear COVID-19 affects your breathing, can I use my iPhone to measure my oxygen levels?
No. A pulse oximeter requires the comparison of readings from *two wavelengths of light to arrive at an oxygen saturation measurement. iPhones have only one and results from apps claiming to accurately determine this should not be trusted. The Centre for Evidence-Based Medicine says: “There is no evidence that any smartphone technology is accurate for the measurement of blood oxygen saturation. The scientific basis of such technologies is questionable. Oxygen saturation levels obtained from such technologies should not be trusted.”

MORE CLINICAL THOUGHTS – DRUG TREATMENT
Is an old antacid, Pepcid (famotidine) is in the news for COVID-19 treatment?
Currently there is only anecdotal data for famotidine’s potential benefit in COVID19 patients. Northwell hospital in New York is conducting a trial that is enrolling patients. This trial’s treatment arm will include hydroxychloroquine + famotidine vs previously treated COVID19 patients. The researchers recognize this is not an ideal trial design but want to get more data. So far the early mention of famotidine is from the use of the drug by one of the researcher’s sister and friends who showed a reduction in symptoms.
I’ve heard that old malaria medications, like chloroquine or hydroxychloroquine, might now be useful, is this true?
We still don’t know for certain. There was early interest in these drugs based on very little data in China and France. Since then, the results of a study out April 21, 2020 funded by the NIH, but yet to be published, shows no benefit in patients treated with hydroxychloroquine compared to those who were not. In fact there is evidence of increased mortality and more cardiac complications. There is a known risk with this drug of QT prolongation which can lead to life threatening cardiac arrhythmias. That said, political discourse around the benefits of the drug continues. There are currently ongoing randomized controlled trials in process which will provide more scientific data in the coming months as to whether hyrdoxychloroquine is beneficial. Until then, the current medical data do not recommend its use unless under a study protocol.

SPEAKING OF GOOD BEHAVIOR – HOW ABOUT MY PETS?
Can I get COVID-19 from my pets or other animals?
The CDC says, probably not. At this time, there is no evidence that animals play a significant role in spreading the virus that causes COVID-19. Based on the limited information available to date, the risk of animals spreading COVID-19 to people is considered to be low. A small number of pets have been reported to be infected with the virus that causes COVID-19, mostly after contact with people with COVID-19. Pets have other types of coronaviruses that can make them sick, like canine and feline coronaviruses. These other coronaviruses cannot infect people and are not related to the current COVID-19 outbreak. However, since animals can spread other diseases to people, it’s always a good idea to practice healthy habits around pets and other animals, such as washing your hands and maintaining good hygiene. For more information on the many benefits of pet ownership, as well as staying safe and healthy around animals including pets, livestock, and wildlife, visit CDC’s Healthy Pets, Healthy People website.
SPEAKING OF BAD BEHAVIOR… WHAT’S THIS ABOUT “DISINFECTANTS”?
I’ve heard I can inject or inhale disinfectant to cure coronavirus, is this true?
No, no, and hell no. Are you crazy? Do NOT inject, ingest, inhale, or bathe in disinfectant, bleach, Tide Pods, Lysol, Listerine, Drano, rubbing alcohol, gasoline, jet fuel, or rat poison. Listen to your real doctor. Thank you.

HOPE AND GRACE
If you have made it this far, time for a reward, something to lighten your day, and acknowledge the human spirit. Find some escape, or perhaps even inspiration, in this collection of works and perspectives gathered from around the world. Please contact me directly if you have come across something that has lifted your heart today. Dr. Eric Weiss
A Letter from the Pandemic: “Am I enough? Is the cold shadow I cast across you and your loved ones enough? Only you…can choose to be the cure to the deeper sickness”. Watch this powerful video from the Global Wildlife Conservation asking about the future we now have the opportunity to choose for ourselves. #extinctionendshere

Check out this crazy new drone footage from San Francisco: New drone footage of shutdown SF eerily evokes film noir (April 26, 2020)
Breathwork as Service : “I asked Spirit often, “How can I be of service to others while utilizing my skills and staying true to who I am?” The message came through that these unprecedented circumstances could invite creative, new ways of supporting others. I felt a calling to share the practice of breathwork. Breathwork, or conscious, controlled breathing, is something that could be accessible to anyone, anywhere”. Kate Coffey is certified in Advanced Spiritual Psychology and Integrative Body Psychotherapy. Learn more at The Truth in Beauty. You can also read more at Women Doing Theology.

HERE’S TO THE KIDS (by Whitney Fleming)
Here’s to the kids who were supposed to get their braces off after two long years, and now have to wait a few more months.
Here’s to the kids who couldn’t wait to get their driver’s license, and now they check daily to see when the DMV will open.
Here’s to the kids who are wondering if there will be any sort of graduation ceremony culminating 13 years of school, or if they will get to attend freshman orientation over the summer at their selected college–or if there will even be a fall semester.
Here’s to the kids who are wondering if they will miss their first time as a camp counselor or employee at the Froyo stand or the internship they worked so hard to get.
Here’s to the kids who were hoping to get their first kiss at the prom.
Here’s to the kids who dreamed of going to States in track or lacrosse or baseball or show choir.
Here’s to the kids who wanted to put themselves out there and try something new this spring.
Here’s to the kids who worked hard all year to come back from an injury.
Here’s to the kids who found their tribe in the band or orchestra or drama department and now feel lost without their people.
Here’s to the shy boy who was working up the courage to ask the new girl out for a movie.
Here’s to the lonely girl who was just starting to make friends in her art class.
Here’s to the kids who have studied all year for their SATs and now sit anxiously wanting to get it over and done with.
Here’s to the kids who have worked hard all year to build up their GPA and now are unsure if their grades count.
And here’s to the kids who miss school because it was their safe place, where they were fed, where someone showed they were valued and loved.
Here’s to the kids whose lives are forever changed, forever branded with the mark of a virus that they do not fear but impacts them greatly.
We talk about big events like proms and graduations and college tours, but it’s not the big things they are missing. It’s the moments woven into these milestones, the imprints of these rites of passage.
We won’t know the long-term damage this will have on our kids for years, so let’s lift them up while we can.
Their grief is real, even if it seems small to us.
Their sadness is justified.
Their lives are changed.
May we remember their perspective is small and their feelings are big.
We can’t give you back the moments, the experience, the time, but we can acknowledge it hurts.
Here’s to the kids.
And lastly,
Thank you, Brad Pitt, for your shout out to Dr. Fauci, but also impressively to healthcare workers, near and far. Enjoy: Brad Pitt as Dr. Anthony Fauci Cold Open – SNL (April 25, 2020).
*****
Yours, in health and resilience,
Eric and the TVD MD team…

