If you’re going through menopause, you’ve probably seen shelves full of supplements promising relief from hot flashes, better sleep, stronger bones, and improved mood. You’re not alone in looking for non-hormonal options — between 40% and 50% of women in Western countries use some form of complementary therapy to manage menopausal symptoms.
The supplement market for menopause is booming, but the reality of clinical evidence tells a more nuanced story. It’s important to understand that “natural” does not automatically mean effective or safe. Many supplements have not been tested with the same rigor as prescription medications, and some can interact with other treatments or carry their own risks.
This article is not a product promotion. It’s a guide to what the research actually shows about popular supplements, so you can have an informed conversation with your doctor. Keep in mind that menopause is not one-size-fits-all: symptom severity, medical history, and treatment goals vary widely from person to person.
What Causes Menopause Symptoms?
Menopause is defined as 12 consecutive months without a menstrual period. The transition leading up to it, perimenopause, can begin years earlier and is driven by fluctuating and eventually declining levels of estrogen and progesterone produced by the ovaries.
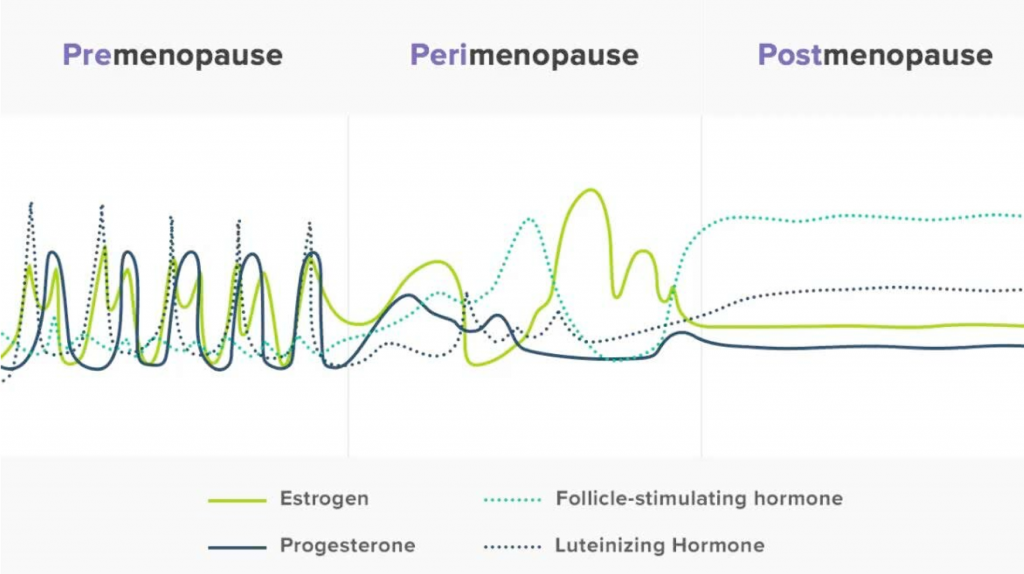
(picture courtesy of Flordis.com.au)
These hormonal shifts cause hot flashes, night sweats, sleep disruption, mood changes, vaginal dryness, brain fog, and joint aches. Genetics, body composition, stress, and diet all influence which symptoms you experience and how severe they are.
Before Trying Supplements: What Patients Should Know
Supplements are not regulated like prescription medications. Ingredient quality, dosing, and labeling accuracy can vary widely. Look for third-party testing seals (USP, NSF, or ConsumerLab), which are ways to ensure the supplements you’re buying contain what the label claims.
Supplements can also interact with medications including antidepressants, blood thinners, hormone therapy, thyroid medications, and breast cancer treatments. Always talk to your doctor before starting a supplement, especially if you have a history of breast cancer, liver or cardiovascular disease, heavy bleeding, osteoporosis risk, or clotting risk.
Hormone therapy remains the most effective treatment for significant perimenopausal and menopausal symptoms. If your symptoms are affecting your quality of life, this is worth discussing at your next visit with your doctor.

Supplements for Menopause: What Does the Evidence Say?
Isoflavones (Soy and Red Clover)
Isoflavones are plant compounds with weak estrogen-like activity, found in soybeans and red clover. Interest grew from the observation that Asian women with soy-rich diets report fewer hot flashes.
What the Research Shows: A JAMA meta-analysis of 62 studies (6,600+ women) found phytoestrogens reduced hot flashes by about 1.3 per day compared to placebo, with a small improvement in vaginal dryness. However, in other studies, placebo groups saw 40–60% reductions in hot flashes on their own, making it hard to isolate a true effect. The typical dose studied is 40–80 mg of isoflavones per day.
Safety: Short-term use appears safe. Moderate soy food intake does not appear to increase breast cancer risk, but the American Cancer Society advises breast cancer survivors to avoid high-dose isoflavone supplements (≥100 mg/day). Women on tamoxifen should be particularly cautious.
Takeaway: Soy foods (tofu, edamame, soy milk) are safe and may modestly help hot flashes. High-dose supplements warrant caution, especially with a breast cancer history.
Creatine
Creatine monohydrate is gaining attention not for hot flashes, but for preserving muscle mass and strength after menopause.
What the Research Shows: A 2026 meta-analysis of 7 randomized controlled trials (608 postmenopausal women) found creatine supplementation produced a small gain in lean mass and improved leg-press strength, but only at doses of 5 g/day or more combined with resistance training. Lower doses without exercise showed no effect. It is still unclear whether creatine is beneficial for prevention of age-related cognitive decline, but some small clinical trials have been promising.
Safety: Creatine was well tolerated across all studies, with no kidney function changes. The most common side effect is minor water retention. Those with pre-existing kidney disease should consult their doctor. Your lab values may show a slight increase in serum creatinine, so you can pause supplementation for 24-48 hours prior to the lab draw to avoid artificially increasing your creatinine levels.
Takeaway: Creatine won’t help hot flashes, but it may support muscle and strength when paired with resistance training (≥5 g/day). It’s inexpensive and has a strong safety profile.
Magnesium
Magnesium is involved in bone metabolism, muscle function, sleep, and mood. Many postmenopausal women don’t get enough from their diet.
What the Research Shows:
- Hot flashes: A pilot study suggested benefit, but a rigorous placebo-controlled trial of 289 women (the N10C2 Alliance trial) found magnesium oxide was no better than placebo. Current evidence does not support magnesium for hot flashes.
- Sleep: A meta-analysis of 3 randomized controlled trials (RCTs) found magnesium reduced the time to fall asleep.
- Mood: One RCT of 126 adults found 248 mg/day of elemental magnesium improved depression and anxiety scores within two weeks.
- Bone health: Women’s Health Initiative data (73,000+ women) showed higher magnesium intake was linked to 2–3% higher bone density, but not fewer fractures. No RCT has shown magnesium supplementation reduces fracture risk.
Safety: Supplemental magnesium can cause diarrhea and cramping, especially magnesium oxide. Better-tolerated forms include citrate and glycinate. The upper limit for supplements is 350 mg/day. Women with kidney disease should use caution.
Takeaway: Magnesium doesn’t treat hot flashes. It may modestly help sleep and mood, and adequate intake supports bone health. The strongest case is for correcting deficiency, not megadosing. Most needs can be met through leafy greens, nuts, seeds, and whole grains. If you suspect you’re not getting enough, a moderate supplement (250–350 mg/day of a well-absorbed form like magnesium glycinate or citrate) is reasonable to discuss with your doctor.
Vitamin D
Vitamin D is essential for calcium absorption and bone health, and deficiency is common in postmenopausal women, particularly those with limited sun exposure, darker skin, or obesity. While vitamin D is not typically marketed as a “menopause supplement,” it’s one of the most important nutrients for postmenopausal health, primarily because of its role in preventing osteoporosis.
What the Research Shows:
Bone health and fractures: Meta-analyses have shown a modest reduction in hip fracture risk with the greatest benefit seen in older women (≥60 years) and those in institutional settings. The Women’s Health Initiative found that calcium plus vitamin D preserved hip bone mineral density and reduced hip fractures in women over 60 and in those who were adherent with supplementation.
Safety: Vitamin D at standard doses (600–1,000 IU/day) is safe. The Institute of Medicine sets the tolerable upper limit at 4,000 IU/day. When combined with high-dose calcium supplements, there is a small increased risk of kidney stones.
Takeaway: Vitamin D is not a treatment for hot flashes or most menopause symptoms, but adequate intake is important for bone health. Most guidelines recommend 600–1,000 IU/day for postmenopausal women, with some experts recommending higher doses to achieve serum 25-hydroxyvitamin D levels above 20–30 ng/mL. Dietary sources include fatty fish, fortified milk, and egg yolks, but many women will need a supplement to reach adequate levels. Talk to your doctor about whether testing your vitamin D level makes sense.
Other Commonly Asked-About Supplements
Black cohosh
Black cohosh is a popular herbal remedy, but the evidence is mixed. Some studies show benefit for hot flashes and overall menopausal symptoms, while others do not. Black cohosh is metabolized by the liver and can interact with many commonly prescribed and over the counter medications (such as Tylenol), with some cases of liver failure as a result of combining it with medications. Please talk to your doctor if you would like to try black cohosh to be sure it is safe for you.
Vitamin E, omega-3 fatty acids, and curcumin
Vitamin E, omega-3 fatty acids, and curcumin (a compound found in turmeric) have shown some early promise for reducing hot flash intensity, but more research is needed. Turmeric is a natural anti-inflammatory, so this could also be beneficial for other conditions such as arthritis.
Evening primrose oil, dong quai, ginseng, and flaxseed
Evening primrose oil, dong quai, ginseng, and flaxseed have not shown reliable benefit for hot flashes in well-designed studies at this time.
When Menopause Symptoms Need Medical Treatment
Supplements are not a substitute for proven treatments when symptoms are moderate to severe. Hormone therapy remains the most effective option for hot flashes, reducing frequency by about 75%. Non-hormonal prescriptions such as SSRIs, SNRIs, and gabapentinoids are also available. If symptoms are significantly affecting your daily life, it’s time to talk to your doctor.
The Bottom Line
Menopause is a universal experience, but no two women go through it the same way and there is no single supplement that works for everyone. As this review shows, most over-the-counter supplements have limited or inconsistent evidence for relieving the hallmark symptoms of menopause, like hot flashes and night sweats. Some, like vitamin D and creatine, may play a supporting role in long-term postmenopausal health when used appropriately, but none are a substitute for proven medical treatments when symptoms are significantly affecting daily life.
The most important step is having the right conversation. A knowledgeable primary care doctor can help sort through the noise, assess individual risk factors, and build a personalized plan that may include lifestyle changes, evidence-based supplements where appropriate, and medical treatments when needed.
At The Village Doctor, our team takes a personalized, evidence-based approach to menopause care. You don’t have to navigate menopause alone.
Angela Jiang, MD; May 2026
OpenEvidence, an AI-powered medical research tool, was used to help draft this post. The author then reviewed and edited the text, cross-referencing NatMed Pro for accuracy.
References
1. Use of Plant-Based Therapies and Menopausal Symptoms: A Systematic Review and Meta-analysis.
The Journal of the American Medical Association. 2016. Franco OH, Chowdhury R, Troup J, et al.SR
2. ACOG Practice Bulletin No. 141: Management of Menopausal Symptoms.
Obstetrics and Gynecology. 2014. Committee on Practice Bulletins—Gynecology This Practice Bulletin was developed by the Committee on Practice Bulletins—Gynecology with the assistance of Clarisa Gracia, MDGuideline
3. Phytoestrogens for Menopausal Vasomotor Symptoms.
The Cochrane Database of Systematic Reviews. 2013. Lethaby A, Marjoribanks J, Kronenberg F, et al.SR
4. American Cancer Society Nutrition and Physical Activity Guideline for Cancer Survivors.
CA: A Cancer Journal for Clinicians. 2022. Rock CL, Thomson CA, Sullivan KR, et al.Guideline
5. American Cancer Society Guideline for Diet and Physical Activity for Cancer Prevention.
CA: A Cancer Journal for Clinicians. 2020. Rock CL, Thomson C, Gansler T, et al.Guideline
The American Journal of Clinical Nutrition. 2019. Touillaud M, Gelot A, Mesrine S, et al.Observational
Journal of the International Society of Sports Nutrition. 2026. Naddafha S, Antonio J, Kreider RB, Stout JR.NewSR
Medicine and Science in Sports and Exercise. 2023. Chilibeck PD, Candow DG, Gordon JJ, et al.RCT
The Journals of Gerontology. Series A, Biological Sciences and Medical Sciences. 2020. Sales LP, Pinto AJ, Rodrigues SF, et al.RCT
Menopause. 2015. Park H, Qin R, Smith TJ, et al.RCT
Supportive Care in Cancer : Official Journal of the Multinational Association of Supportive Care in Cancer. 2011. Park H, Parker GL, Boardman CH, Morris MM, Smith TJ.Clinical Trial
12. Oral Magnesium Supplementation for Insomnia in Older Adults: A Systematic Review & Meta-Analysis.
BMC Complementary Medicine and Therapies. 2021. Mah J, Pitre T.SR
13. Role of Magnesium Supplementation in the Treatment of Depression: A Randomized Clinical Trial.
PloS One. 2017. Tarleton EK, Littenberg B, MacLean CD, Kennedy AG, Daley C.RCT
The American Journal of Clinical Nutrition. 2014. Orchard TS, Larson JC, Alghothani N, et al.Observational
Endocrine Practice: Official Journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists. 2020. Camacho PM, Petak SM, Binkley N, et al.Guideline
16. The 2022 Hormone Therapy Position Statement of the North American Menopause Society.
Menopause. 2022.
17. Management of Menopausal Symptoms: A Review.
The Journal of the American Medical Association. 2023. Crandall CJ, Mehta JM, Manson JE.Review
18. NatMed Pro: https://naturalmedicines.therapeuticresearch.com/Home/ND
Call The Village Doctor at (650) 851-4747 or Contact us to learn more about the practice.


